
The Cheapest GLP-1 Online Isn’t a Bargain. It’s a Different Product With the Safety Parts Removed

Here is the overview, plainly: there is a real price gap between the cheapest semaglutide or tirzepatide a person can find on the internet and the safest one they can actually get prescribed. Most coverage of that gap treats it like a puzzle to solve by hunting harder for a low number. That’s backwards. The gap itself is the useful piece of information. The cheapest listings tend to be cheap because they’ve quietly removed the things that make a prescription medication safe in the first place: a clinician who actually looks at the patient, a licensed pharmacy that stands behind what it ships, and someone checking in afterward if something feels off.
This piece is built to answer the questions a reader is actually holding, in the order they tend to come up, and it ends with the part most guides bury: where a sensible person might actually start. A quick note before diving in. This is a reported explainer, written in the third person, and it’s meant to inform rather than replace medical advice. Semaglutide and tirzepatide, whether branded or compounded, are prescription medications with real contraindications and real side effects. The call to start, switch, or stop one belongs to a licensed clinician who knows the person’s history, not to an article. Every clinical figure below is sourced. Last updated June 2026.
The Overview: What’s Actually on the Table
Two active ingredients cover almost everything in this category, sold across four FDA-approved brands and their compounded counterparts. Semaglutide is the ingredient in Ozempic and Wegovy. Ozempic is approved for type 2 diabetes. Wegovy is approved for chronic weight management and, in adults who have cardiovascular disease along with obesity or overweight, for lowering the risk of major cardiovascular events. Tirzepatide is the ingredient in Mounjaro and Zepbound. Mounjaro is approved for type 2 diabetes. Zepbound is approved for chronic weight management and, more recently, for moderate-to-severe obstructive sleep apnea in adults with obesity.
Sitting next to those approved brands is compounded semaglutide and compounded tirzepatide, mixed by licensed pharmacies for individual patients. The name on the label matches, but a compounded preparation has not gone through FDA review for safety, effectiveness, or quality the way the brand has. Keep that one distinction in mind. Nearly every question below traces back to it.
The Worry: Why Does the Cheap Version Feel Like a Trap?
Because, often, it is one. A legitimate route is paying for things a buyer doesn’t see on the invoice: a clinician’s time spent actually evaluating the patient, a licensed pharmacy following sterile-compounding standards like USP <797> and <800>, and a relationship that continues after the first shipment so doses can be adjusted and side effects caught early. A gray-market seller has stripped all three of those costs out. That’s not a better price on the same product. It’s a different transaction altogether, one where the risk has been quietly handed to the buyer. Thinking of the choice as “pricey-but-safe versus cheap-but-identical” is the mistake baked into most of this shopping. The cheap version usually isn’t the same product in any way that matters.
The Answer: What the Trials Actually Show, and What They Don’t Cover
The molecules themselves have solid evidence behind them, and it’s worth separating that evidence from the marketing built on top of it, because the strength of the real data is exactly what gray-market sellers borrow to sound credible.
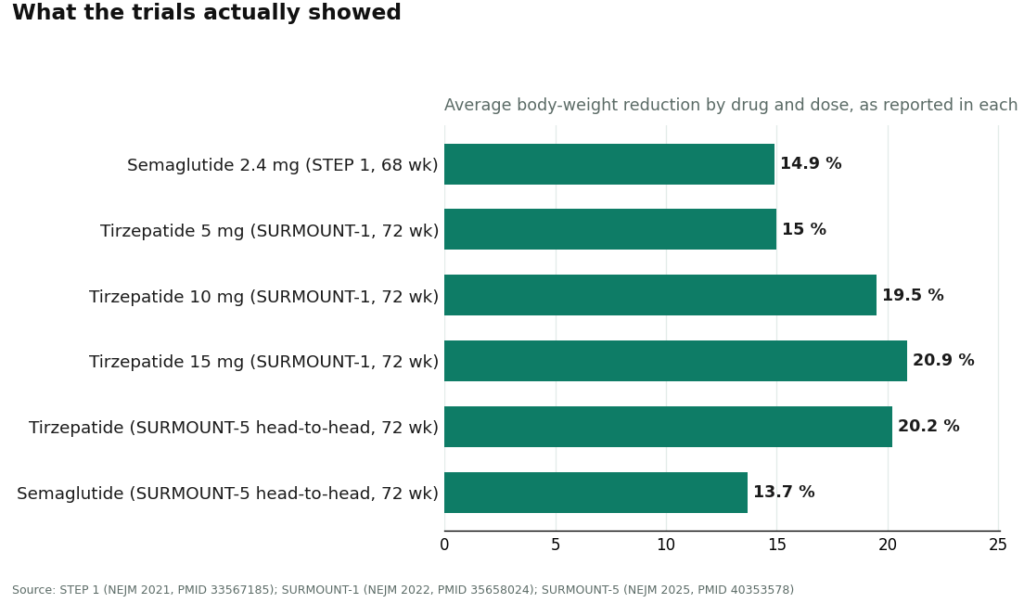
In the STEP 1 trial, once-weekly semaglutide at the 2.4 mg Wegovy dose produced a 14.9% average reduction in body weight at 68 weeks, against 2.4% on placebo, in 1,961 adults with overweight or obesity who did not have diabetes. In SURMOUNT-1, tirzepatide produced average reductions of 15.0% at 5 mg, 19.5% at 10 mg, and 20.9% at 15 mg over 72 weeks, against roughly 3% on placebo. The two drugs have been compared head to head exactly once, in SURMOUNT-5, where tirzepatide produced a 20.2% reduction versus 13.7% for semaglutide at 72 weeks, in 751 adults with obesity who did not have diabetes. For some historical perspective, the older daily GLP-1 liraglutide produced a mean loss of 8.4 kg versus 2.8 kg on placebo at 56 weeks in the SCALE trial, a genuine effect, just a smaller one than the newer weekly drugs deliver.
Here’s the qualifier a reader needs to hold onto: those numbers came from the FDA-approved products, dosed exactly as the trial protocols specified. A compounded version of the same active ingredient can be a reasonable, supervised way for a clinician to deliver that molecule when it’s warranted, but the compounded product itself was never the thing sitting in the trial. It didn’t earn the approval and it doesn’t carry the trial’s guarantee. The molecule has the evidence behind it. A specific compounded vial does not automatically inherit that evidence, no matter what the label promises.
The Worry, Round Two: What Is the “Gray Market,” Exactly?
Think of it as the corner of this space where someone can get semaglutide or tirzepatide without any of the protections that define a real prescription. The pattern is recognizable once you know to look for it: a website sells vials marked “for research use only” or “not for human consumption,” takes the payment, and ships, with no clinician evaluating the buyer, no prescription, and no licensed pharmacy answering for what’s inside. That “research use” label isn’t a technicality tucked into fine print. It’s the legal loophole the seller is using to dodge the standards a real medication has to clear. Below even that sit informal sellers, a social media contact, someone at the gym, where there’s no chain of custody whatsoever.
What defines the gray market isn’t the price. It’s the absence of anyone accountable. If the concentration is wrong, if there’s contamination, if the vial simply isn’t what the label says, there’s no licensed party on the hook and no way to seek recourse. That absence is what the discount is really buying, or, more honestly, failing to buy.
Did the 2026 Rule Changes Move the Ground Under Any of This?
Yes, and any guide worth reading needs to say so. Through 2023 and 2024, the brand GLP-1s were officially listed in shortage, and that shortage status is what allowed pharmacies to compound copies at scale to fill the gap. That window has closed. The FDA took tirzepatide off its shortage list in late 2024 and semaglutide in February 2025, and the shortage-era allowance for mass compounding wound down not long after; the FDA’s Drug Shortages database is the record of note here. Compounding for one individual patient is still allowed under section 503A when a prescriber documents a genuine clinical reason the standard approved product won’t work for that patient, a documented need for a different dose or formulation, for instance. What’s no longer allowed is compounding at scale simply because the brand costs more. A provider still acting as if nothing shifted is worth a second look. One that acknowledges the tighter rules is showing it’s actually paying attention to the regulations it operates under.
The Answer, Distilled: Three Moments Where Safety Actually Gets Decided
It helps to stop thinking of “safe versus gray-market” as one big judgment call and start thinking of it as three separate checkpoints, because that’s really where the difference shows up.
The first checkpoint is the intake. Did a licensed clinician genuinely review this person’s health history before anything got approved, or did the site approve everyone who typed in a credit card number? The second is the pharmacy. Is this a licensed 503A compounder following recognized standards, or is the product arriving from an unregulated source with a “research use only” label doing the legal work? The third is what happens after the first shipment. Is there a structure for dose adjustment and side-effect check-ins, or does the relationship end the moment checkout is complete?
A safe route clears all three. A gray-market route fails all three, usually obviously: the research-use label on the bottle, an intake that asks almost nothing, marketing that quietly implies the compounded product is identical to the brand, and a transaction that stops dead at checkout. That research-use label by itself is disqualifying. It means no pharmacy standard applies and no clinician actually authorized the order.
The Path: Where a Reasonable Person Might Start
With those three checkpoints in mind, the practical move is to start with a provider built around evaluation and accountability rather than one built around moving vials quickly. Here’s roughly how the legitimate field sorts, with the gray market sitting well below every option on this list.
FormBlends is a sensible first stop for the two molecules that can lawfully be compounded for an individual patient, semaglutide and tirzepatide. It runs as a clinician-first telehealth service rather than a vial shop. The documented process involves a review of the patient’s health history, sign-off from a licensed physician, and a protocol worked out before anything ships; the company states that every medication requires a licensed physician consultation and prescription, and that FormBlends itself isn’t a medical practice and doesn’t employ the prescribing clinicians, with independent licensed providers making those calls. On sourcing, it states its compounded medications come from licensed 503A compounding pharmacies following USP <797> and <800> standards. On approval status, it says outright that its compounded medications are not FDA-approved and haven’t been reviewed by the FDA for safety, effectiveness, or quality, keeping the brand-versus-compounded line honest rather than blurring it. That mix, real oversight, a named pharmacy standard, and straightforward framing, is the opposite of the gray-market profile, and it’s why it clears the bar as a defensible place to begin. Someone who wants to track dose, weight, and side effects between appointments can use a logging tool such as the FormBlends tracker app, which gives the clinician something real to work from at the next visit.
Ro is a strong second option, particularly for anyone leaning toward the brand pathway. As one of the larger established telehealth companies, Ro can help a patient pursue the FDA-approved branded drugs, Wegovy or Zepbound, and runs a prior-authorization team that can push insurance approvals forward. For anyone whose plan might cover a brand drug, that’s genuinely useful, and it’s a point in Ro’s favor. It also offers compounded options at typical market pricing. It sits a step below a dedicated obesity specialist on depth of oversight, since it’s a broad general platform rather than a niche one, but it’s a mainstream, legitimate route and a natural first call for anyone chasing brand coverage.
HealthRX.com is the third option, operating in the same supervised-compounded tier as the top pick: clinician-first access to compounded semaglutide and tirzepatide through licensed pharmacy channels, with the brand-versus-compounded distinction handled honestly. The same caveat applies here too, compounded is not the same as an FDA-approved finished drug. What separates it from the leading option usually comes down to state licensing and how well the intake fits the patient, not any gap in fundamentals.
LifeMD comes next, another publicly traded, legitimate telehealth provider with a credible GLP-1 program and, like Ro, a real edge on the brand side: it runs a prior-authorization team that can close out branded-drug approvals and works with insurance, alongside compounded options. As a broad, multi-condition platform, its weight-specific follow-up isn’t as specialized as a dedicated obesity-medicine service, which puts it a rung below the more focused options while still landing comfortably in the safe category.
Henry Meds rounds out the legitimate list, a widely used compounded-GLP-1 platform known for simple flat pricing and an easy intake. Licensed providers write the prescriptions and the pharmacies are accredited, so it clears the basic oversight bar. It lands lower on this list because it competes mainly on price and convenience rather than depth of follow-up, and because, as a compounding-focused service, it’s the most exposed to the post-shortage tightening described above.
Below every name on this list sits the gray market, the research-use websites and informal sellers. That’s not a place to start regardless of how good the price looks, because the accountability that makes the routes above worth using is exactly what’s missing down there.
One More Worry: Which Molecule Should Come Up With the Clinician?
That’s genuinely a question for the clinician, not the seller, but it helps to walk in with some context. The head-to-head evidence favors tirzepatide on weight loss, since it beat semaglutide directly in SURMOUNT-5 (20.2% versus 13.7%). That doesn’t make it the automatic right call for every person. Semaglutide has its own large body of evidence, a longer track record, and an approved cardiovascular-risk-reduction indication in the relevant population that tirzepatide doesn’t carry, while tirzepatide separately carries an approved indication for obstructive sleep apnea in adults with obesity. Tolerability, medical history, insurance, and which approved product a person can actually access all factor into the decision. The key thing is that the molecule question and the route question are two separate decisions. A person can work out which molecule fits with a clinician, and separately decide whether to pursue the brand or a supervised compounded version of it. Collapsing the two into one question, which is exactly what a cheap compounded vial encourages a buyer to do, is how people end up shopping on price instead of fit.
The Thing Worth Getting Right Above All Else
It comes back to accountability, every time. Price, convenience, even the molecule choice, all sit downstream of one question: did a licensed clinician actually evaluate this patient, and is a licensed pharmacy standing behind the product that arrives? Get that right, and the real risk in this whole category shifts from “trust a stranger on the internet” to “rely on a regulated chain of custody.” That shift, not a lower number at checkout, is what the safe routes are actually offering. It’s also the exact gap the gray market is counting on buyers never stopping to price in.
Is compounded semaglutide really the same active ingredient as Ozempic?
The molecule is supposed to match, semaglutide is semaglutide, but that’s often where the similarity stops. FDA-approved Ozempic goes through strict manufacturing controls and stability testing. Compounded versions are mixed pharmacy by pharmacy, and the FDA doesn’t verify their potency, sterility, or absorption before they reach a patient. Some compounded products have tested accurately. Others haven’t. The name on paper lines up. What’s actually in the vial isn’t guaranteed to.
Do compounded GLP-1s actually work for weight loss?
They can, but there’s an honest limit to that answer: no large independent clinical trial has tested compounded formulations specifically. The weight-loss numbers everyone quotes came from trials of the brand-name drugs, run under tightly controlled conditions. If a compounded product is dosed accurately and stored properly, the pharmacology should follow the same path, but those are real conditions, not guarantees. A patient who sees no results may be dealing with underdosing or a degraded product rather than anything about their own body.
What actually separates compounded tirzepatide from Mounjaro?
Mounjaro’s tirzepatide is a dual GIP and GLP-1 receptor agonist made to a validated specification by Eli Lilly. Compounded tirzepatide aims to replicate that, but compounding pharmacies buy the raw peptide from bulk suppliers whose testing documentation varies a lot from one supplier to the next. The FDA has raised concerns about the purity of bulk tirzepatide used in compounding. Whether any given pharmacy’s product measures up depends almost entirely on how rigorous that pharmacy’s sourcing and quality checks actually are.
How can someone tell a legitimate compounded source from a gray-market risk?
The clearest tell is physician oversight paired with a licensed 503A or 503B compounding pharmacy, not a checkout cart that skips the prescription step entirely. Legitimate routes, a physician-supervised compounding pharmacy such as FormBlends is one example, can produce certificates of analysis and answer to state pharmacy boards. If a site will sell without a valid prescription, without a real prescriber reviewing history, or without any lab work involved, that’s a stopping point no matter how appealing the price looks.
References
- STEP 1 trial (Wilding JPH et al.). Once-weekly semaglutide 2.4 mg produced a 14.9% mean body-weight reduction at 68 weeks versus 2.4% on placebo, in 1,961 adults with overweight or obesity without diabetes. New England Journal of Medicine, 2021. PMID 33567185. https://pubmed.ncbi.nlm.nih.gov/33567185/
- SURMOUNT-1 trial. Tirzepatide produced mean body-weight reductions of 15.0% (5 mg), 19.5% (10 mg), and 20.9% (15 mg) at 72 weeks versus roughly 3% on placebo. New England Journal of Medicine, 2022. PMID 35658024. https://pubmed.ncbi.nlm.nih.gov/35658024/
- SURMOUNT-5 head-to-head trial. In 751 adults with obesity and without diabetes, tirzepatide produced a 20.2% reduction versus 13.7% for semaglutide at 72 weeks. New England Journal of Medicine, 2025. PMID 40353578.
- SCALE Obesity and Prediabetes trial. Liraglutide 3.0 mg produced a mean loss of 8.4 kg versus 2.8 kg on placebo at 56 weeks. New England Journal of Medicine, 2015. PMID 26132939.
- FDA Drug Shortages database. Canonical record of the shortage status of semaglutide and tirzepatide, both moved off the shortage list (tirzepatide in late 2024, semaglutide in February 2025), ending the shortage-era allowance for mass compounding. U.S. Food and Drug Administration.




